Sickle cells
From haematologyetc.co.uk
Also known as: drepanocytes [drepanon = sickle]
Derivation: Derivation: descriptive – shaped like the farming tool “sickle”
Appearance The abnormal cells are very elongated and crescent shaped with dense bodies and characteristic sharp-ends.

Images Sickle cells: The appearance is distinctive, note the dense elongated shape without central pallor, a typical sickle erythrocyte must have a curved shape and sharp ends, although intermediate or incomplete forms will also be present. Context is important with features of increased new cell production (polychromatic cells or nRBCs), other damaged or distorted cells (target, contracted or boat shaped cells), and features of hyposplenism. Always consider whether this be a compound heterozygote of sickle haemoglobin and another variant.
Significance
The appearance indicates that the cells express the mutated gene for sickle haemoglobin (HbS), either in homozygous form (HbSS) or as a compound with another abnormal beta haemoglobin form. The number of these abnormal cells should not necessarily be considered an indicator of severity, but increased numbers of abnormal cells and polychromasia (or nucleated red cells) often occur during sickle crises.
Pitfalls
Sickle cells are distinctive and typical, the "sharp ends” and curved shape distinguish these cells from elliptocytes or other elongated cells. The context of partial forms, boat-shaped cells and damaged cells adds to diagnostic confidence. However, typical sickle cells can be infrequent, and the question of whether a second haemoglobinopathy coexists should always be asked (look for features of HbSC disease, or of co-existent thalassaemia).
Causes
| Conditions with sickle haemoglobin |
|---|
| Sickle cell disease (HbSS): The typical disorder (features as described above) |
| Sickle cell/haemoglobin C disease (SC disease): may be difficult to distinguish from typical sickle cell disease. Look for more prominent target cells and/or boat-shaped cells as well as branched SC poikilocytes. Typical sickle cells, nucleated red cells, polychromasia, and features of splenectomy are less prominent. |
| Sickle/beta thalassaemia: Morphological distinction from uncomplicated sickle cell disease may not be possible, but suspect this if there is significant microcytosis and hypochromia, and target cells. Sickle cells may be less frequent. |
| Heterozygous (sickle cell trait): There may be sickle cells if subjected to profound hypoxia, but this is very uncommon. Cells with boat-like shape may be found, but many individuals have normal blood film appearances. |
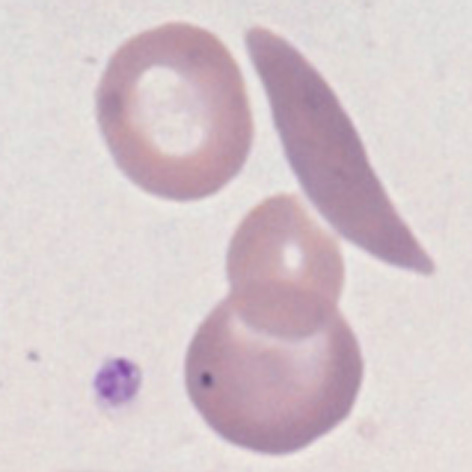
Clinical Image 1: There is only one truly sickle cell, developing forms are however prominent with either “boat form” or more sickle-like intermediate forms. Polychromasia and contracted cells are also prominent. Sickle cells can be much less frequent. Clinical condition: sickle cell disease (HbSS)
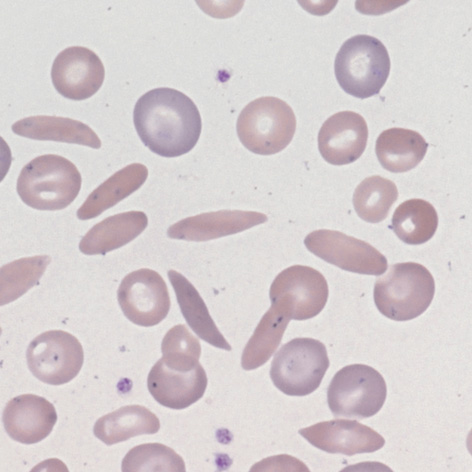
Clinical Image 2: The sickle cells in this field are numerous although few are “perfect examples” - note the variability of form shown. There is also a nucleated red cell and many contracted cells present. Clinical condition: sickle cell disease (HbSS)
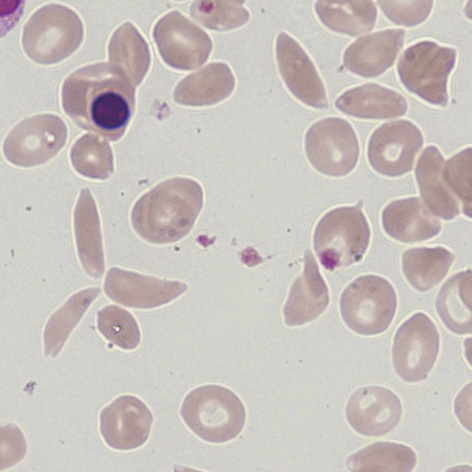
Clinical Image 3: Sickle cells are visible within the “usual background” of target cells and contracted cells. The beta thalassaemia is not immediately apparent in terms of hypochromia since the majority of cells have abnormal form, however there is marked microcytosis (compare with the nuclear size of the small lymphocyte). Clinical condition: sickle cell disease with beta thalassaemia
Pathobiology
The sickle shape derives from the tendency for Haemoglobin S to polymerise into a linear form when oxygen concentration is low. This polymerisation causes the characteristic distortion of the cell.
The sickling process is initially reversible, but secondary damage to the red cell caused by repeated sickling causes intracellular dehydration and damage. This eventually results in cells that have "irreversible" sickle morphology, accompanied by other damaged or abnormal cellular forms, particularly target cells, boat-shaped forms and contracted cells. On blood films the reversibly sickled cells rapidly revert to normal morphology during preparation, so only irreversibly sickled cells will be detected.