Ovalocytes: Difference between revisions
From haematologyetc.co.uk
No edit summary |
No edit summary |
||
| Line 12: | Line 12: | ||
[[File: | [[File:Ova1.png|180px||link=]] | ||
Revision as of 15:10, 20 March 2023
Derivation: latin ovum - egg
Appearance.
An erythrocyte that is rounded, but which has a length that exceeds its diameter is oval. Although the word can be synonymous with an ellipse, in morphological usage the term ovalocyte is used when cell length is less than twice the diameter the cell.
Image 1Image 1 An ovalocyte is a red cell which is regular and rounded but is also elongated. The term ovalocyte can be applied to cells where the length is greater than the width, but is not yet twice the width (at which point the cell is more often referred to as an elliptocyte)
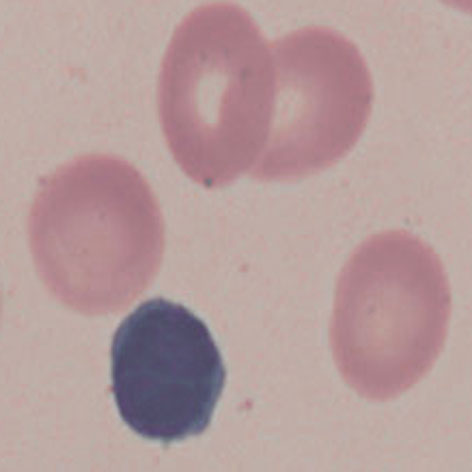
Image 2 There are many different contexts for ovalocytes (see causes). In this case an enlarged and ovoid cell is shown together with a hypersegmented neutrophil a feature of megaloblastic states (most commonly vitamin B12 or folate deficiency).
Significance
Morphologically detectable macrocytosis will generally have an underlying cause. Therefore attention is required to identify this - morphological evidence of any accompanying disease should actively be sought. Most frequently these causes are B12 or folate deficiency, myelodysplasia, or liver disease.
Pitfalls
Where cell fragments are present in addition to macrocytes (this may occur for example in severe vitamin B12 or folate deficiency) this may reduce the overall mean cell volume (MCV) given by automated counters even when the non-fragmented cells are large, this can be a particular issue in megaloblastic anaemia. Also remember that reticulocytes may be 20-25% larger than normal red cells, so polychromatic cells should not be confused with macrocytes.
Causes
| Physiological or artefact |
|---|
| 1. Reticulocytes are larger than mature erythrocytes so MCV is higher |
| 2. Red cell agglutination may result in apparent elevation of overall mean cell volume detected by automated analysers |
| Impaired cell division (nutritional or metabolic) |
| 1. Vitamin B12 deficiency (most commonly due to impaired absorption) |
| 2. Folic acid deficiency (most commonly dietary deficiency) |
| Impaired cell division (drug) |
| 1. Cytotoxic e.g. hydroxycarbamide |
| 2. Immunosuppressive e.g. azathioprine |
| Defective cell formation |
| 1. Most frequently myelodysplasia (also seen in congenital dyserythropoiesis, aplastic anaemia or post stem-cell transplant) |
| Other causes |
| 1. Alcohol and liver disease: excess cell membrane lipid |
| 2. Hypothyroidism. Likely caused by reduced cell division |
| 3. Drugs and medication, causing macrocytosis through various mechanisms |
Clinical Examples
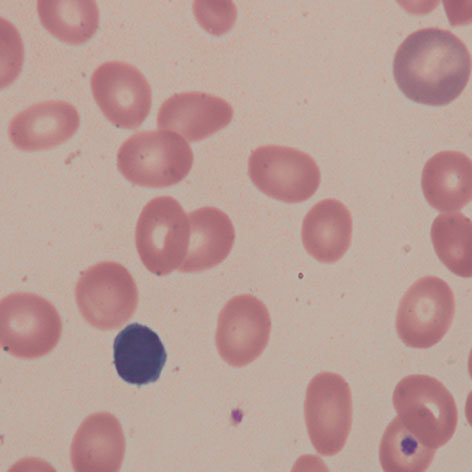
Clinical Image 1: The nucleus of the small lymphocyte provides a reference to judge erythrocyte size – this reveals that almost all the erythrocytes shown here are macrocytes. Note here that the majority have an oval shape “oval macrocytes”. An obvious exception being the truly huge polychromatic erythrocyte (upper right corner) which has a round shape. Clinical disorder: folate deficiency
Clinical Image 2: This film has a more varied cell size with some very large cells, but others of normal or small size. Nonetheless the macrocytes are highly significant. In this case the additional hypersegmented neutrophil indicates the underlying megaloblastic state – some small or even fragmented red cells can occur in severe B12 or folate deficiency reflecting fragile red cells. Clinical disorder: folate deficiency
Pathobiology
Where cell division is impaired the maturing erythrocytes undergo fewer cycles of division and so emerge from the marrow as larger cells. We tend to associate severe macrocytosis with nutritional deficiency affecting cell division (vitamin B12 or folate deficiency); less severe macrocytosis may result from metabolic effects on cell division (e.g. hypothyroidism or occasionally chronic disease), or due to intrinsic impaired cell maturation (myelodysplasia). However, macrocytosis may also arise as a result of increased membrane lipid e.g. in liver disease (most particularly alcoholic liver disease, Zeives Syndrome, or cirrhosis) in this case the macrocytes can be very large.
Significance For ovalocytes that are large, consider: oval macrocytes of megaloblastic states, and the very large (stomatocytic) ovalocytes that are part of of S.E.Asian ovalocytosis. In these cases the additional diagnostic blood appearances are crucial. Where ovalocytes are not enlarged they generally form part of a spectrum of cells e.g. in hereditary elliptocytosis or as part of the dyserythropoietic spectrum in a range of disorders (myelodysplasia, iron deficiency etc). Pitfalls Ovalocytes should be distinguished from other elongated forms (elliptocytes or pencil cells) and can arise as part of the spectrum of elliptocytes where they may be better considered as part of that context. Particularly look for those forms that have particular diagnostic significance (see below) Causes INHERITED DEFECTS S.E.Asian Ovalocytosis A specific disorder that results from structural and functional defects of the band 3 protein causing ovalocytes with a stomatocytic appearance.\ MEGALOBLASTIC STATES Look for characteristic oval macrocytes in the context of typical hypersegmented neutrophils and other features of these disorders AS PART OF A SPECTRUM OF ABNORMAL CELLS Ovalocytes may form as the first stage in elliptocyte formation – consider whether the cells are simply early elliptocytes Ovalocytes and elliptocytes may be infrequent forms in a range of disorders, in those conditions it is probably best to focus on the dominant features of the film
Clinical Image 1 A large ovalocyte within the context of normally sized red cells. Note also the slit like central pallor of many of the cells. Image: S.E.Asian ovalocytosis Clinical Image 2 Multiple oval-shaped cells in the context of general macrocytosis (compare with the nucleus of the included normal small lymphocyte). Image: B12 deficiency Clinical Image 3 More severe megaloblastic anaemia with very prominent large macrocytic cells. In this case the overall fragility of the developing abnormal erythrocytes has also produced small fragmented cells that cause an apparent reduction in the overall MCV. Image: B12 deficiency
Pathobiology Ovalocytes in inherited or dyserthropoietic disorders arise by similar mechanism to elliptocytes having an unstable cytoskeleton that allows them to be deformed by shear-stress; in this case there are a range of forms with different severity. In some instances however they may arise because of a particular defect - the classic ovalocyte arises in S.E.Asian ovalocytosis where the transmembrane protein "band 3" is defective at its binding site with other elements of the erythrocyte cytoskeleton - causing a relatively rigid cell structure. The defect is widespread in S.E.Asian populations and may provide resistance to invasion of the erythrocyte by malarial parasites.