Fragmented cells
From haematologyetc.co.uk
(schistocytes)
Derivation: “schistos” [divided]
Appearance
Irregularly shaped red cell fragments, it is useful to distimguish between fragments that are very asymmetrical with sharp projections; and the more rounded fragments that have a different clinical significance.
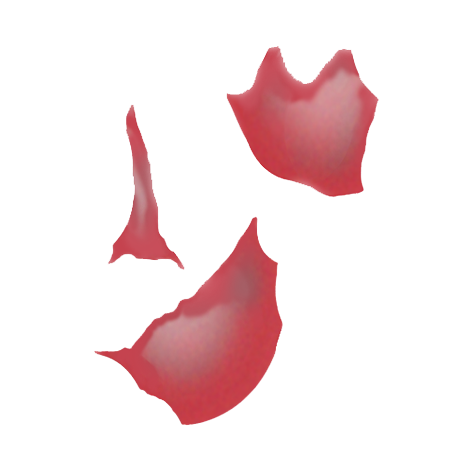
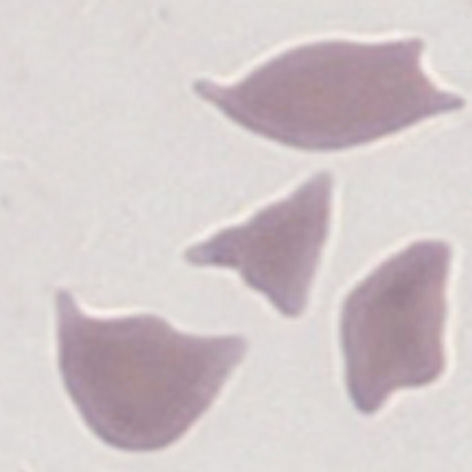
Images 1 These are the sharp fragmented forms that typically arise from fibrin-shearing of erythrocytes and may be regarded as the end stage of the same process that leads to keratocyte formation.
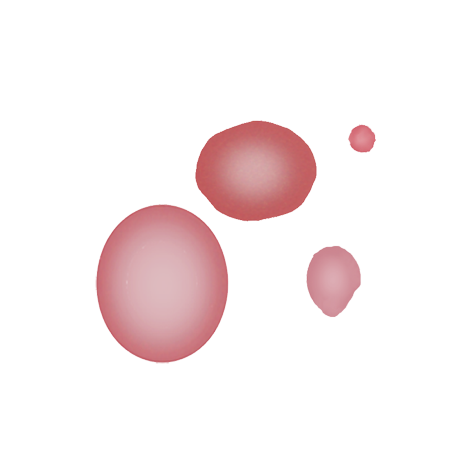
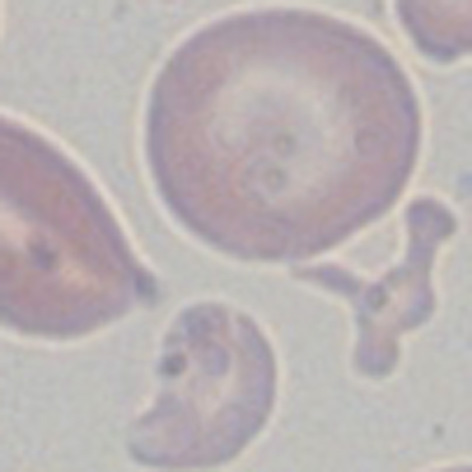
Images 2 More blunt or rounded fragments can arise in a range of disorders where there is membrane instability or damage.
Significance
Fragmented cells are not found in normal blood. Sharp fragments may reflect “microangiopathic” damage - this form of fragmentation may therefore represent a medical emergency and should be reported immediately. More rounded fragments arise in significant dyserythropoiesis (such as severe myelodysplasia, membrane disorder or megaloblastic states), these are also important to diagnosis, but have a different origin.
Pitfalls
Fragments are a “final pathological form” arising in a variety of processes. It is important when reporting these cells therefore, to reflect whether the film appearances represent a disorder where fragmentation is the primary pathological process (generally sharp ended), or whether the fragments are a reflection of cell fragility in a wider haematological disorder (generally rounded).
Causes
| Shearing processes (produce sharp fragments) |
|---|
| Fibrin strands |
| Microangiopathic haemolysis: thrombotic thrombocytic purpura, haemolytic uraemic syndrome, pregnancy associated - HELLP syndrome (haemolysis, elevated liver enzymes and low platelet count), or pre-eclampsia. |
| Disseminated intravascular coagulation |
| Myelofibrosis |
| Turbulent blood flow |
| Valvular heart disease |
| Haemangiosarcoma |
| Fragile erythrocytes |
| Congenital dyserythropoiesis |
| Myelodysplasia |
| Severe haematinic deficiency |
| Severe membrane disorder |
Clinical examples
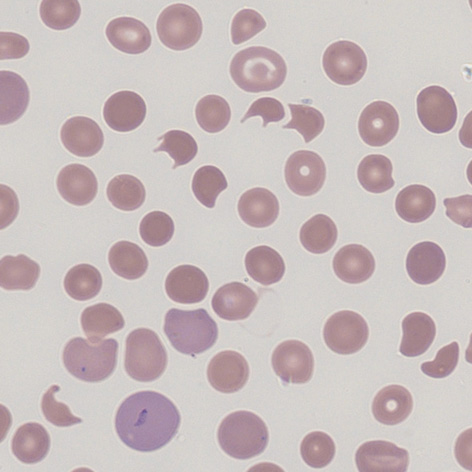
Clinical Image 1: Early fragmentation – note that for many cells there is still a resemblance to keratocytes. Other cells with membrane loss are also present (particularly spherocytes) and platelets are not seen. There is also polychromasia as the marrow responds to red cell loss. Clinical condition: thrombotic thrombocytopenic purpura.
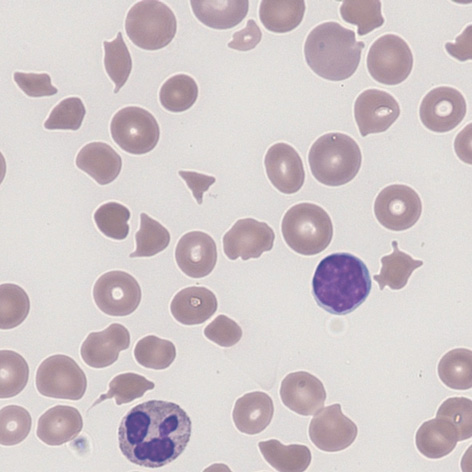
Clinical Image 2 Established fragmentation –the damaged red cells are very angular having undergone several cycles of damage. The resemblance to keratocytes is now much less marked. Clinical condition: thrombotic thrombocytopenic purpura.
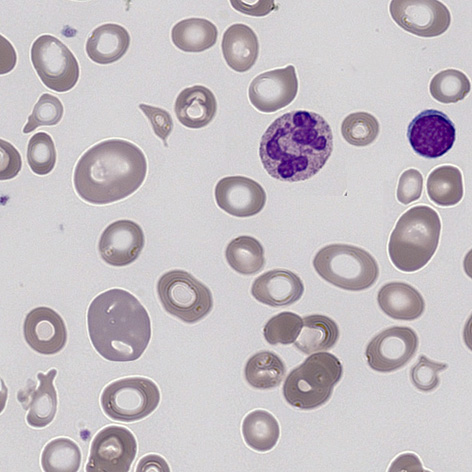
Clinical Image 3 "Blunt fragments” - note that the context is different with few normal cells present, and that the fragments have a rounded and often quite varied shape reflecting membrane fragility. Clinical condition: megaloblastic anaemia (deficiency of vitamin B12).
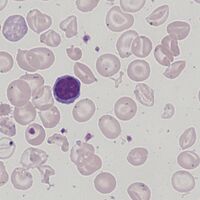
Clinical Image 4 "Blunt fragments” - like the previous example the fragments form part of a broad distribution of abnormal cell shapes that are rounded and often with irregular projections reflecting their abnormal fragility and formation. Clinical condition: thalassaemia intermedia.
Pathobiology
Fibrin deposition in small vessels causes mechanical “shearing” of red cells (this may also be a feature of severely turbulent flow of blood e.g. damaged heart valves). The fragmented cells arising from this mechanism should be viewed as a more severely damaged form of the keratocyte (which will often also be present). A second more rounded form of fragment arises in an intrinsically fragile red cell, where it is thought to represent membrane instability – here the fragments appear different and keratocytes are not generally present - look instead for features of severe inherited membrane disorder or dyserthropoietic states.