Gallery of early trophozoites: Difference between revisions
From haematologyetc.co.uk
No edit summary |
No edit summary |
||
| Line 8: | Line 8: | ||
---- | ---- | ||
<span style="font-size:90%">''' ''P.falciparum'' '''</span></br> | <span style="font-size:90%">''' ''P.falciparum'' '''</span></br> | ||
<span style="font-size:90%">Small delicate rings, | <span style="font-size:90%">Small delicate rings, and these '''may be the only forms seen in some patients at diagnosis'''. Infected red cells have normal (or slightly crenated) appearance.</br> | ||
<gallery heights=200px widths=200px> | <gallery heights=200px widths=200px> | ||
| Line 18: | Line 18: | ||
---- | ---- | ||
<span style="font-size:95%">''' ''P.vivax'' '''</span></br> | <span style="font-size:95%">''' ''P.vivax'' '''</span></br> | ||
<span style="font-size:90%">Rings begin as small forms, but become larger | <span style="font-size:90%">Rings begin as small forms, but become larger asociated with enlarged distorted red cells as they develop. Schüffner's dots will become present | ||
<gallery heights=200px widths=200px> | <gallery heights=200px widths=200px> | ||
| Line 24: | Line 24: | ||
File:PVET2g.jpg|<span style="font-size:80%">Early ring form with faint dots</span>|link={{filepath:PVET2g.jpg}} | File:PVET2g.jpg|<span style="font-size:80%">Early ring form with faint dots</span>|link={{filepath:PVET2g.jpg}} | ||
File:PVET3g.jpg|<span style="font-size:80%">Llarge thickened ring trophozoite</span>|link={{filepath:PVET3g.jpg}} | File:PVET3g.jpg|<span style="font-size:80%">Llarge thickened ring trophozoite</span>|link={{filepath:PVET3g.jpg}} | ||
File:PVET4g.jpg|<span style="font-size:80%">Distorted ting trophozoite and red cell, marked | File:PVET4g.jpg|<span style="font-size:80%">Distorted ting trophozoite and red cell, marked Schüffner's dots</span>|link={{filepath:PVET4g.jpg}} | ||
</gallery>" | </gallery>" | ||
---- | ---- | ||
<span style="font-size:90%">''' ''P.ovale'' '''</span></br> | <span style="font-size:90%">''' ''P.ovale'' '''</span></br> | ||
<span style="font-size:90%">Ring form is retained but enlarges, red cells may develop fimbriation and enlarged ovoid form with James dots. | <span style="font-size:90%">Ring form is retained but enlarges, red cells may develop fimbriation and enlarged ovoid form with visible James' dots. | ||
<gallery mode="traditional" widths=200px heights=200px> | <gallery mode="traditional" widths=200px heights=200px> | ||
| Line 38: | Line 38: | ||
---- | ---- | ||
<span style="font-size:95%">''' ''P.malariae'' '''</span></br> | <span style="font-size:95%">''' ''P.malariae'' '''</span></br> | ||
<span style="font-size:95%"> | <span style="font-size:95%">Infected red cells are generally infrequent. Early trophozoites are small in normal or small erythrocytes, and may have central chromatin dot, elongation or angular forms. | ||
<gallery mode="traditional" widths=200px heights=200px> | <gallery mode="traditional" widths=200px heights=200px> | ||
Revision as of 13:26, 27 November 2024
Navigation
Go Back
General Comments: At the very earliest point all trophozoites appear as ring forms and species differences are very difficult to distinguish - some "species specific" features may appear as parasites mature toward late trophozoite stages.
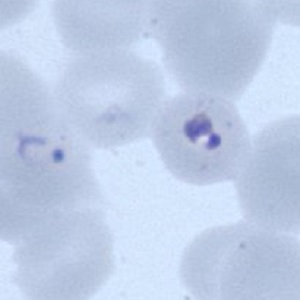
P.falciparum
Small delicate rings, and these may be the only forms seen in some patients at diagnosis. Infected red cells have normal (or slightly crenated) appearance.

Fine ring form

Double dot form and normal ring

Accolé and double dot forms

Multiple parasite form




"
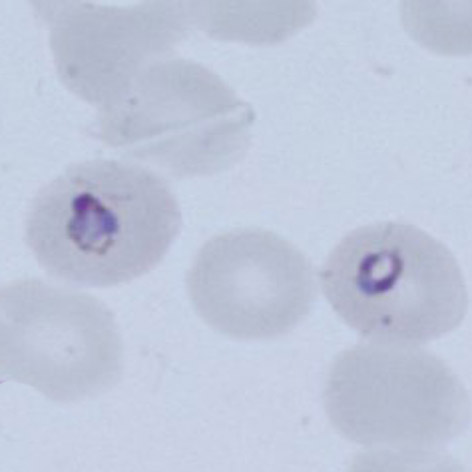
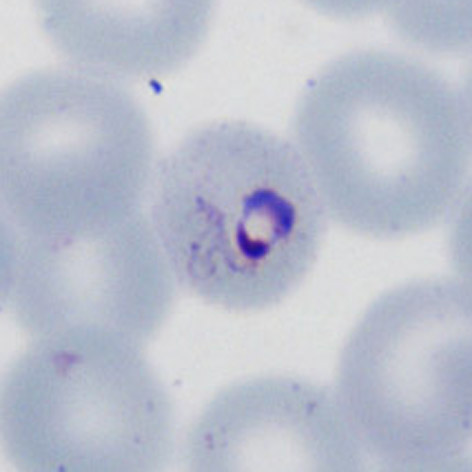
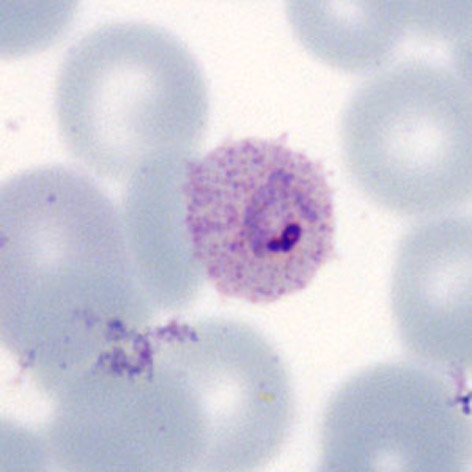
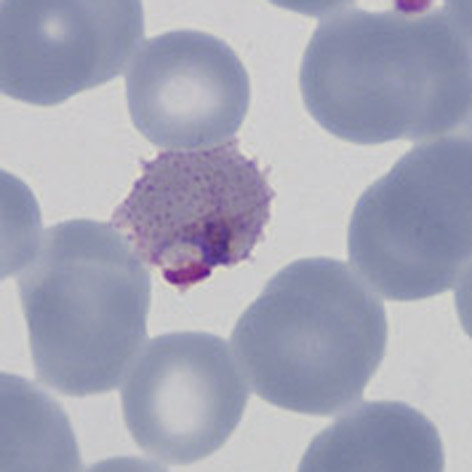
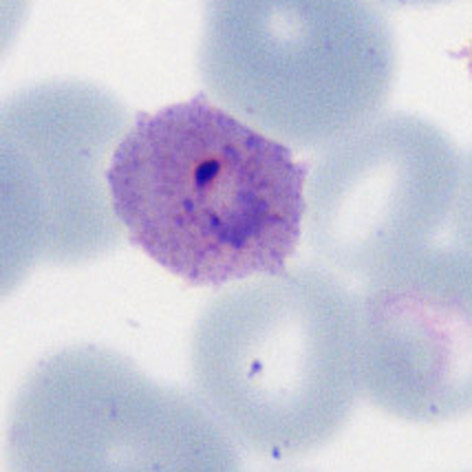
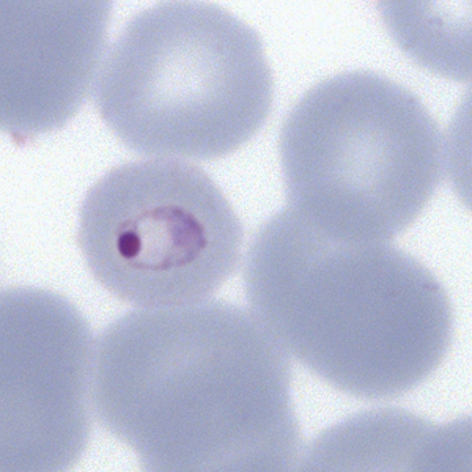
P.vivax
Rings begin as small forms, but become larger asociated with enlarged distorted red cells as they develop. Schüffner's dots will become present

Early ring form

Early ring form with faint dots

Llarge thickened ring trophozoite

Distorted ting trophozoite and red cell, marked Schüffner's dots




"
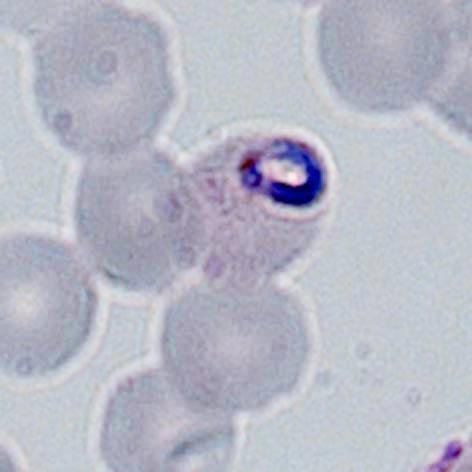
P.ovale
Ring form is retained but enlarges, red cells may develop fimbriation and enlarged ovoid form with visible James' dots.

Early ring form

Ring with dots/fimbriation

faint Ziemann's dots

Ring early ovoid change
"
P.malariae
Infected red cells are generally infrequent. Early trophozoites are small in normal or small erythrocytes, and may have central chromatin dot, elongation or angular forms.

Ring form in small red cell

The central chromatin dot

Early elongation, Stinton's dots

Early angularity of form


"
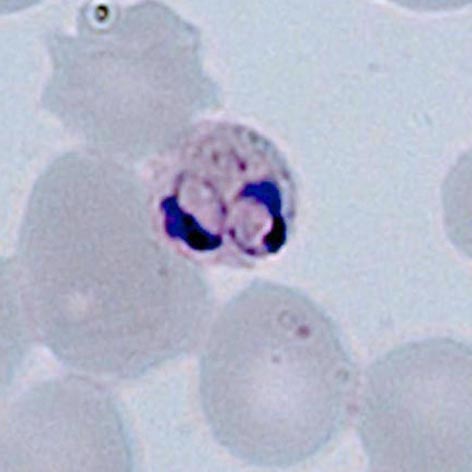
P.knowlesi
At the early trophozoite stage an infection by P.knowlesi resembles that of P.falciparum and the number of infected cells amy be high. Forms found may also resemble P.falciparum with parasites that have double chromatin dots, multiply infected red cells, or accolé forms. This may create diagnostic difficulty in cases where only early trophozoites are present. Later forms however begin to resemble parasites of P.malariae and these should be specifically sought where infections arise in geographical areas associated with this parasite.

Fine early rings

Double dot (right)

Accolé form

Multiple infection