Biology of the gametocyte: Difference between revisions
From haematologyetc.co.uk
No edit summary |
No edit summary |
||
| Line 32: | Line 32: | ||
<gallery mode="nolines" widths="200px" heights="220px" > | <gallery mode="nolines" widths="200px" heights="220px" > | ||
File: | File:PFGc.jpg|A typical curved gametocyte of ''P.falciparum''|link={{filepath:PFGc.jpg}} | ||
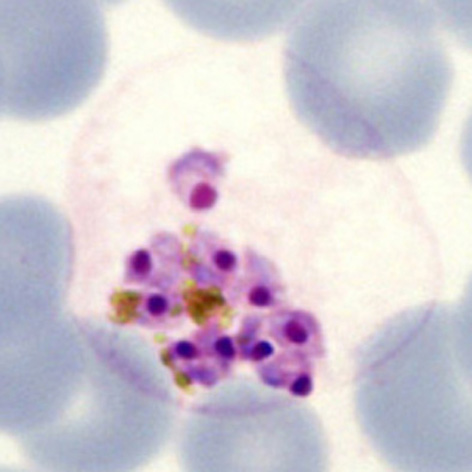
File:Schizontreal4.jpg|Mature schizont releasing merozoites|link={{filepath:Schizontreal4.jpg}} | File:Schizontreal4.jpg|Mature schizont releasing merozoites|link={{filepath:Schizontreal4.jpg}} | ||
File:Schizontreal4.jpg|Mature schizont releasing merozoites|link={{filepath:Schizontreal4.jpg}} | File:Schizontreal4.jpg|Mature schizont releasing merozoites|link={{filepath:Schizontreal4.jpg}} | ||
Revision as of 13:53, 31 May 2024
Navigation
(click blue highlighted text to return to page)
Malaria main index
>Basic malaria biology
>>This page: Biology of the schizont
| The gametocyte pathway |
The gametocyte is the committed sexual form of the malarial parasite. Gametocytes have either male or female form (a higher percentage are female). However this form should probably be considered as “dormant” in blood, since they do not develop further until ingested by a mosquito - following a temperature drop in the mosquito foregut the gametocytes then rapidly form the active sexual form – either a single female gamete or 8 male gametes (see section on re-infection of the mosquito).
Generally male gametocytes (microgametocytes) are smaller then the female form (macrogametocytes). This is shown in the image below:
| Morphological features and relevance |
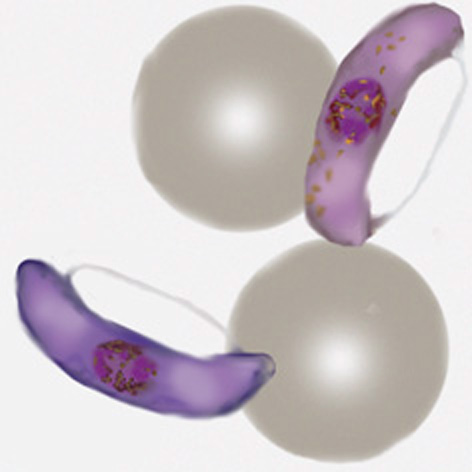
(1) P.falciparum – typically elongated or “banana” shaped forms
(2) P.malariae – typically small and neat rounded forms
(3) P.vivax – typically very large and often irregular
(4) P.ovale – typically sightly enlarged and may be fimbriated
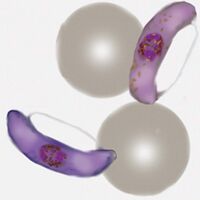
A typical curved gametocyte of P.falciparum
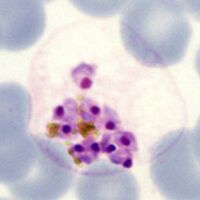
Mature schizont releasing merozoites
Mature schizont releasing merozoites
Mature schizont releasing merozoites
→ Click for the gametocyte gallery
| Relevance of gametocytes to clinical biology |
Following treatment of malaria these forms may persist (depending on the nature of the treatment) particularly in the first week but sometimes up to 28 days (unlike the asexual forms that generally disappear more rapidly).