Biology of the gametocyte: Difference between revisions
From haematologyetc.co.uk
No edit summary |
No edit summary |
||
| (29 intermediate revisions by the same user not shown) | |||
| Line 4: | Line 4: | ||
<span style="font-size:90%">>[[Malaria_Index|Main Malaria Index]]''</span></br> | <span style="font-size:90%">>[[Malaria_Index|Main Malaria Index]]''</span></br> | ||
<span style="font-size:90%">>>[[Malaria_Biology|Malaria Biology Index]]''</span></br> | <span style="font-size:90%">>>[[Malaria_Biology|Malaria Biology Index]]''</span></br> | ||
<span style="font-size:90%">>>>[[ | <span style="font-size:90%">>>>[[Biology_of_the_gametocyte|Gametocyte Biology]]</span></br> | ||
---- | ---- | ||
| Line 14: | Line 14: | ||
|colspan="1" style = "font-size:100%; color:black; background: white"|<span style="color:navy></span> | |colspan="1" style = "font-size:100%; color:black; background: white"|<span style="color:navy></span> | ||
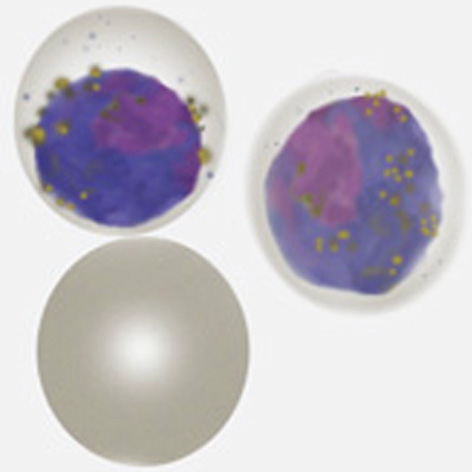
The | The sexual form of the malarial parasite has either male or female form (a higher percentage are female). Generally male gametocytes (microgametocytes) are smaller then the female form (macrogametocytes). They are effectively “dormant” in blood and only develop further when ingested by a mosquito (the temperature drop in the mosquito foregut rapidly activates them to a single female gamete or 8 male gametes (see section on re-infection of the mosquito). | ||
---- | ---- | ||
{| class="wikitable" style="border-style: | {| class="wikitable" style="border-style: none; border-width: 2px; border-color: gainsboro; color:black" | ||
|colspan="1" style = "font-size:100%; color:black; background: | |colspan="1" style = "font-size:100%; color:black; background: gainsboro |'''Morphological features and relevance''' | ||
|} | |} | ||
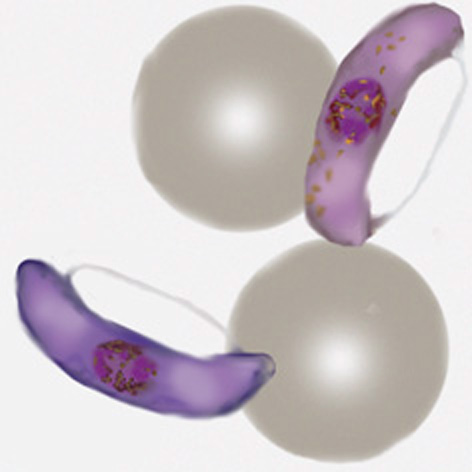
Gametocytes (like schizonts) are the final mature form of parasites in the blood, consequently they have metabolised all haemoglobin in order to grow. The red cell is therefore now simply a membrane that surrounds the parasite without any red colour, and with prominent malaria pigment that represents the metabolised haem iron. The appearance of gametocytes however does vary according to species and this can aid morphological species identification</br></br> | |||
( | ''' ''P.falciparum'' ''' In this species the gametocytes have a "rod" shape which may be constricted by the remaining red cell membrane to form a curved shape (often described as banana-shaped). | ||
<gallery mode="nolines" widths="150px" heights="150px" > | |||
File:PFGc.jpg|link={{filepath:PFGc.jpg}} | |||
File:PFG4.jpg|link={{filepath:PFG4.jpg}} | |||
</gallery></br></br> | |||
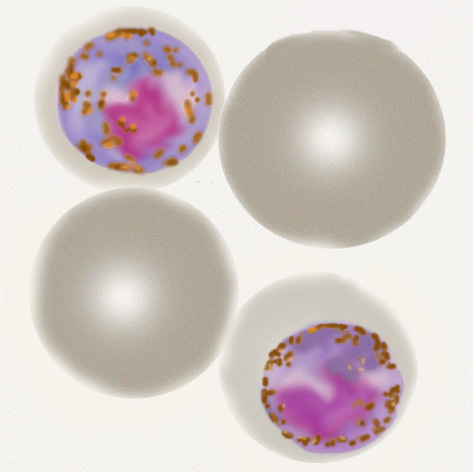
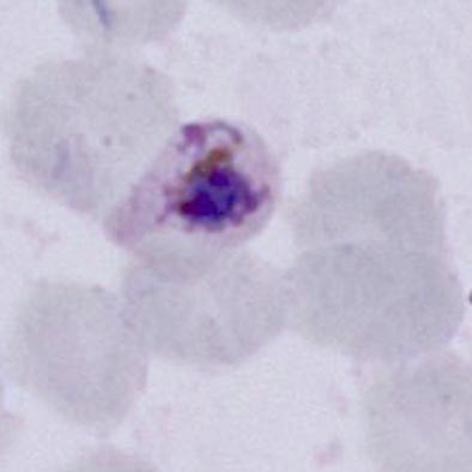
''' ''P.malariae'' ''' | |||
Like other stages in this species the red cell containing the parasite is not enlarged or distorted and may be small. Parasites are typically small and neat with rounded form that do not fill the red cell. | |||
<gallery mode="nolines" widths=" | <gallery mode="nolines" widths="150px" heights="150px" > | ||
File: | File:PMGc.jpg|link={{filepath:PMGc.jpg}} | ||
File: | File:PMG1.jpg|link={{filepath:PMG1.jpg}} | ||
File: | </gallery></br></br> | ||
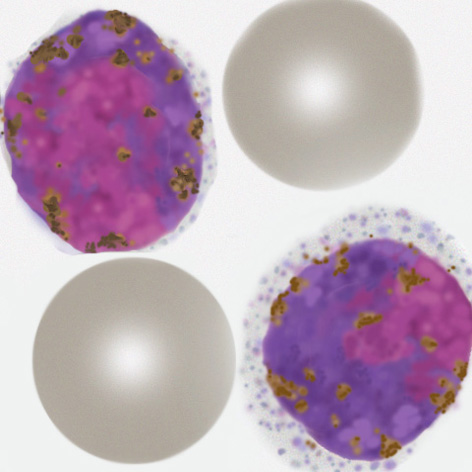
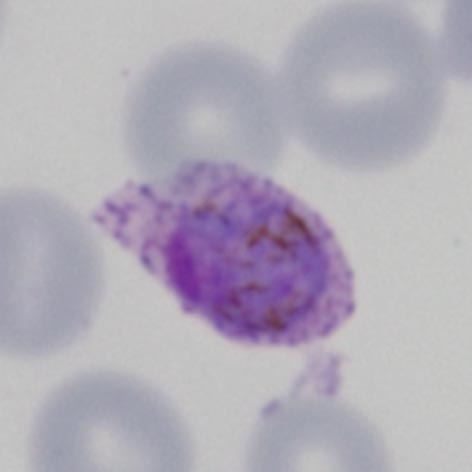
File: | ''' ''P.vivax'' ''' | ||
</gallery> | Typically these are very enlarged (significantly larger than normal red cells) often retaining the irregular shape that devlelops in ''P.vivax'' during the trophozoite stage. | ||
</br><gallery mode="nolines" widths="150px" heights="150px" > | |||
< | File:PVGc.jpg|link={{filepath:PVGc.jpg}} | ||
File:PVG1.jpg|link={{filepath:PVG1.jpg}} | |||
</gallery></br></br> | |||
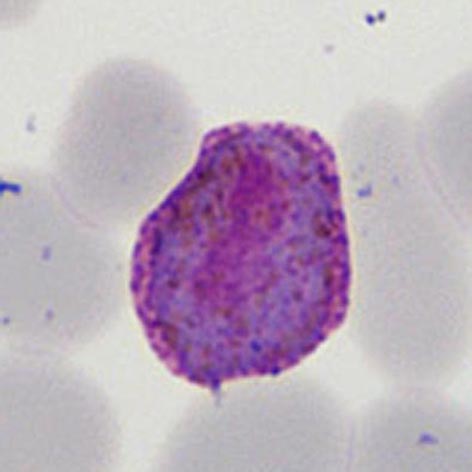
''' ''P.ovale'' ''' | |||
Like other species the trophozites retain the species-specific features acquired during the late trophozoite phase, they may appear sightly enlarged, often ovoid, and have fimbriation. | |||
</br><gallery mode="nolines" widths="150px" heights="150px" > | |||
File:POGc.gif|link={{filepath:POGc.gif}} | |||
File:POG4.jpg|link={{filepath:POG4.jpg}} | |||
</gallery></br></br> | |||
''' ''P.knowlesi'' ''' | |||
These gametocytes tend to be small like ''P.malariae'' but less neat and well formed, | |||
</br><gallery mode="nolines" widths="150px" heights="150px" > | |||
File:PKGc.jpg|link={{filepath:PKGc.jpg}} | |||
File:PKG1.jpg|link={{filepath:PKG1.jpg}} | |||
</gallery></br></br> | |||
---- | ---- | ||
{| class="wikitable" style="border-style: | {| class="wikitable" style="border-style: none; border-width: 2px; border-color: gainsboro; color:black" | ||
|colspan="1" style = "font-size:100%; color:black; background: | |colspan="1" style = "font-size:100%; color:black; background: gainsboro |'''Relevance of gametocytes to clinical biology''' | ||
|} | |} | ||
Latest revision as of 20:08, 7 November 2024
Navigation
>Main Malaria Index
>>Malaria Biology Index
>>>Gametocyte Biology
Biology of the Gametocyte
|
The sexual form of the malarial parasite has either male or female form (a higher percentage are female). Generally male gametocytes (microgametocytes) are smaller then the female form (macrogametocytes). They are effectively “dormant” in blood and only develop further when ingested by a mosquito (the temperature drop in the mosquito foregut rapidly activates them to a single female gamete or 8 male gametes (see section on re-infection of the mosquito).
Gametocytes (like schizonts) are the final mature form of parasites in the blood, consequently they have metabolised all haemoglobin in order to grow. The red cell is therefore now simply a membrane that surrounds the parasite without any red colour, and with prominent malaria pigment that represents the metabolised haem iron. The appearance of gametocytes however does vary according to species and this can aid morphological species identification P.malariae Like other stages in this species the red cell containing the parasite is not enlarged or distorted and may be small. Parasites are typically small and neat with rounded form that do not fill the red cell. P.vivax Typically these are very enlarged (significantly larger than normal red cells) often retaining the irregular shape that devlelops in P.vivax during the trophozoite stage. P.ovale Like other species the trophozites retain the species-specific features acquired during the late trophozoite phase, they may appear sightly enlarged, often ovoid, and have fimbriation. P.knowlesi These gametocytes tend to be small like P.malariae but less neat and well formed,
|