Irregularly contracted cells
From haematologyetc.co.uk
Derivation: A simple term describing cell shape
Appearance
Dense cells that have a distorted and often irregular outline; central pallor is generally absent and haemoglobin staining may be irregular within the cell. Most often there is a spectrum of forms present.
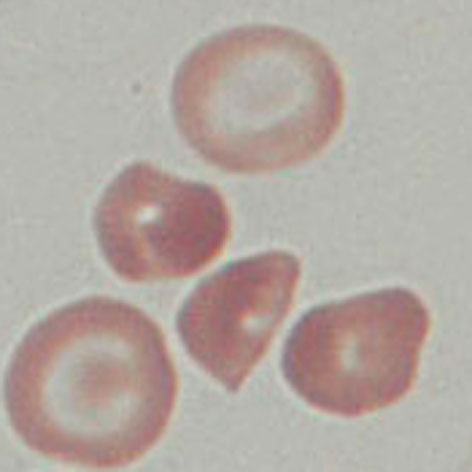
Characterised by an irregular outline and diminished or absent central pallor. As this is a damaged cell type the appearances can be very variable. But generally the haemoglobin staining-density will be irregular, and that the condensed and dehydrated cells will have reduced size. The other cells present are also important since these cells generally arise in the context of other abnormal cell types – often indicating the underlying pathology (in this case target cells).
Significance
The irregular contraction implies damage to haemoglobin within the red cell often accompanied by cellular dehydration and membrane damage; however, the appearance is not specific and represents the final stage of several distinct pathological processes. In most cases the cause of the appearance will not be an acute event that requires urgent intervention, although the possibility of acute oxidative damage to red cells should be considered.
Pitfalls
The principle important distinction is from the spherocyte which may also co-exist; a predominantly spherocytic appearance has a very different pathogenesis and significance so careful attention to morphology is important.
Causes
| Abnormal haemoglobin forms (look for associated typical cell forms)
| |
|---|---|
| Sickle cell disease (including variant forms) | |
| Haemoglobin C disease | |
| Unstable haemoglobin | |
| Thalassaemias | |
| Pathological causes | |
| Infiltrated bone marrow: (look also for white cell precursor cells): consider leukaemia, myelofibrosis or infiltrating solid tumour. | |
| Conditions associated with erythroid expansion: haemoglobinopathy (particularly thalassaemia); severe membrane disorder with haemolysis; dyserythropoietic anaemias | |
Clinical Examples
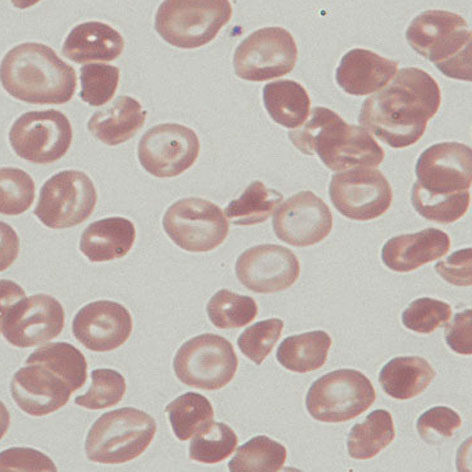
Clinical Image 1: The most eye-catching cell here is the target cell (with many nice examples). However, look at the remaining cells on the field and it can be easily appreciated hat most are small, condensed, and have irregular cell outline and often density. These are irregularly contracted cells. Clinical condition: Haemoglobin C disease
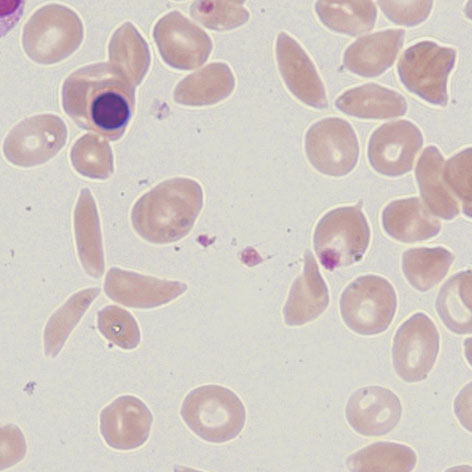
Clinical Image 2: The irregularly contracted cells are not the most prominent feature since the eye is drawn to the sickle and boat shaped cells, as well as the nucleated red cell. However, a closer look shows that the cellular background contains many condensed and irregular cells – perhaps less abnormal than in the Haemoglobin C example (above), but nonetheless a prominent cell form here. Clinical condition Sickle cell disease
Clinical Image 3: This film has much to look at – there are frequent target cells, two nucleated erythrocytes, and general hypochromia. Again however a closer look at the remaining cells shows that many are very small, condensed and irregular. Clinical condition: beta thalassaemia intermedia
Pathobiology
The contracted and hyperdense appearance of the affected erythrocytes reflects damage to both haemoglobin and membrane. This is most clearly apparent where the damaged haemoglobin becomes contracted away from the membrane (and may form particular hemi-ghost cells). In cases of haemoglobinopathy (particularly HbC or HbS) the appearance reflects repeated cycles of damage and cellular dehydration.